What do you need to know about having a Hysterectomy?
Does Hysterectomy cure all your problems? Please read our new blog...
You may silence your body by chopping off the uterus, but the ROOT CAUSE of your period problem still exists and gets worse like a clicking time bomb waiting to explode...

Dr Disha Sridhar
I am a Gynaecologist Obstetrician ( MD, DNB OBGYN )with an emphasis on INTEGRATIVE MEDICINE.

So today, I address a very important question ⁉
Do we need a period if childbearing is over or not required?
Now and then, I see a client who is sick of her period cycle and wants to get rid of it simply because it's too inconvenient, painful, unpredictable, unmanageable or annoying.
Last week a friend called me telling me how tired she was with the adenomyosis pain and wanted to get rid of the uterus, aka HYSTERECTOMY SURGERY. She says that childbearing is complete, and none of the hormonal methods suits her, simply driving her crazy. And this lady is in her early 40s, younger than me! And before I could get over that, another client told me that her teenage daughter is so sick of her periods that she wants to get rid of her cycles and, if required, uterus! That breaks my heart, and I thought it was time to do this post... And I understand that; I have been there too.
But now, after falling in love with my period cycle, I feel sad to see young women ready to do anything, go under the knife, and sacrifice their uterus to get some relief from their periods. At one point in time, I also absolutely hated my cycle and wanted to get rid of it; In fact, I always viewed it as a liability until I could heal my relationship with my cycle and get my life back!
Do you also tend to see your period as a pain, an Inconvenience or something to fear each month?
While This Mentality is typical, and I participated in myself for the better part of my life, it puts us in victim consciousness, as if something is happening to us. We have no control over it, but nothing could be further from the truth. You have much more control over your periods and fertility than you were made to believe! By Understanding what’s happening during each phase of our cycle with our Hormones, we become empowered to have habits that not only improve our physical health but also level up us on mental, emotional and spiritual levels.
I know everyone now, and then one article will come in the media, claiming that there's no reason for modern-day women to have a period and that we would be better off and healthier if we didn't bleed every month, or that it would simply be convenient! There are pills which can be taken continuously to skip bleeding indefinitely.
It's genius for the human species to bio-hack the system and makes life convenient, but it doesn't mean it's good for our long-term health. Of course, there are conditions where this may be medically indicated, and it's a personal choice, but I want to make you aware that what if there is a better way... Nature is infinitely more intelligent than we are and gave us the gift of our menstrual cycle to protect our long-term health. Interfering with the intelligent female body design comes with real side effects and health dangers.
Ovulation and menstruation have played an essential role in safeguarding our health for decades and protecting us from heart disease, osteoporosis, breast disease and Alzheimer's. Our menstrual cycle is so critical to our overall health and well-being that the #AmericanCollegeofObstetriciansandGynecologists has stated that menstruation is the fifth vital sign, just as crucial as pulse, temperature, respiratory rate and blood pressure.
I receive a lot of questions regarding hysterectomies, which is a gynecological topic. What are the effects of a hysterectomy on a woman's hormones? And how can you minimize the adverse effects and symptoms of a hysterectomy? Is it even necessary for a woman to have a hysterectomy in the first place?
First and foremost, I want to acknowledge that a hysterectomy can save a woman's health, as I learned when I started as a gynecologist decades ago. Hysterectomy is a standard procedure for uterine cancer and many non-cancer-related diseases (fibroids, heavy bleeding, cramping, etc.). But after seeing so many women suffering from the effects of the surgery, I delved into this surgical procedure. I asked myself what the underlying causes led to a hysterectomy and the after-effects of the surgery.
What's a hysterectomy, and why do women have them?
The term "hysterectomy" comes from the Latin word "hyster," which means "womb."
Hysterectomy is a abdominal surgical procedure that removes all or part of the uterus and the cervix, fallopian tubes, and ovaries in some cases. It sounds straightforward, but removing reproductive parts adversely affects women's mental health as they lose the ability to reproduce and affect the menstrual cycle.
But we need to understand why hysterectomies are performed on women?
Many hysterectomies are for causes other than cancer or life-threatening situations. Primarily for "benign" purposes. Even benign conditions have an impact on women's health, both mentally & physically.
So, what are the conditions that a hysterectomy has traditionally treated?
The following are benign (quality-of-life affecting) conditions:
- Uterine fibroids: Noncancerous development within the uterus muscle is the most common reason for hysterectomy (also known as leiomyomas). They can cause severe bleeding and pain, although they typically go unnoticed.
- Abnormal uterine bleeding: Fibroids or other uterine problems might cause this.
- Endometriosis: This is a condition in which the tissue that borders the uterus appears outside the uterus, on the ovaries, fallopian tubes, or elsewhere in the pelvis. It's frequently linked to pelvic and menstrual pain.
- Uterine prolapse, pelvic prolapse, and other pelvic support issues can be a reason for a hysterectomy.
- Chronic pelvic pain (severe cramping, etc.)
- Adenomyosis: It is a condition when the uterus lining tissue develops inside the uterus walls, producing severe bleeding and agony.
The following are medical (life-threatening) conditions:
— Gynecological cancers (cervical cancer, ovarian cancer, uterine cancer, endometrial cancer): Hysterectomy surgery is a prophylactic measure for women with a family history of cancer as it helps to get rid of this deadly condition.
— Cervical dysplasia: This condition causes abnormal cells to form on the cervix, typically discovered during a routine PAP smear.
— Endometrial hyperplasia is a thickening of the uterine lining that isn't cancer, but some women can progress to cancer. Estrogen dominance, or excessive oestrogen without enough progesterone, can cause it.
— Complications during childbirth (rupture of the uterus).
— Uncontrollable bleeding or a uterine infection.
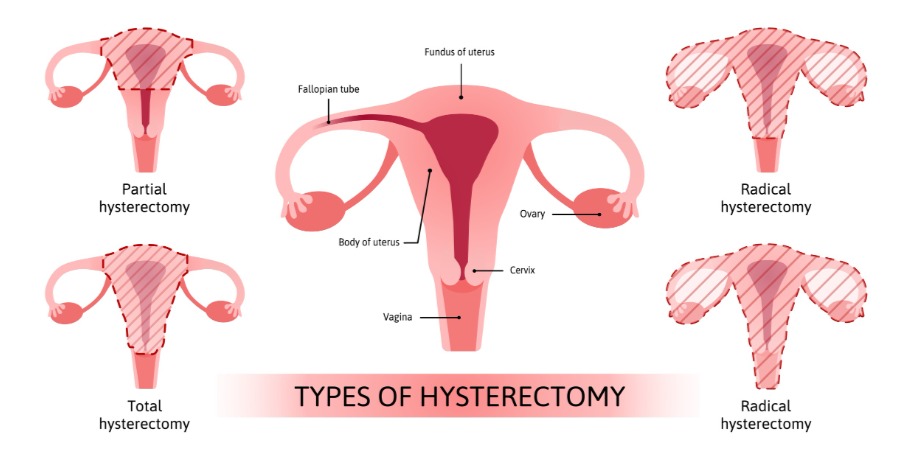
After understanding the reasons for having a hysterectomy, let us understand the types:
Hysterectomies are done depending on the patient's condition:-
— Partial hysterectomy: It's also known as subtotal or supracervical hysterectomy. This procedure removes the upper section of the uterus while leaving the cervix intact.
— In a total hysterectomy, the entire uterus and the cervix are removed.
— In Radical hysterectomy, the entire uterus, the tissues along the sides of the uterus, cervix and the top part of the vagina are removed often to keep uterine cancer at bay.
— Removal of ovaries is called oophorectomy, and removing fallopian tubes is called salpingectomy. Removing both ovaries & fallopian tubes is known as a salpingo-oophorectomy. Some women have them removed as a preventative measure against ovarian cancer.
— Abdominal hysterectomy is the most common type of hysterectomy. It involves an incision in the abdominal wall/belly area and removing the uterus.
— The uterus is removed through the vaginal canal in a vaginal hysterectomy.
Are hysterectomies a hereditary or a genetic condition?
While a hysterectomy is a surgical treatment, it is not genetically determined. Some illnesses or risk factors, such as cancer, fibroids, and endometriosis, are unquestionably influenced by heredity and genetics. It can result in a hysterectomy.
Now we need to understand the side effects and long-term risks before having a hysterectomy because it will affect the reproductive capabilities of a woman.
Side-effects:-
— Menopause symptoms: The removal of ovaries before menopause causes the loss of the protection of estrogen against osteoporosis, heart disease risks and dementia. It may be the right decision for a woman, especially if her risk for ovarian cancer is high.
— Although the evidence is inconsistent, decreased libido and sexual function are often side effects of hysterectomy.
— Following a hysterectomy, some women suffer a sense of loss, melancholy, or depression. It could be related to a woman's perception of how the operation will affect her womanhood (inability to have children if she is still of childbearing age) and sexuality.
— Pelvic organ prolapse, structural pain, urinary incontinence, bowel dysfunction, pelvic organ fistula formation, and sexual function issues are only a few of the long-term complications of hysterectomy.
— Urinary incontinence, structural pain, and the risk of prolapse.
— Bowel dysfunction
— Women under 50 who have had a hysterectomy may have a higher risk of cardiovascular disease later in life.
Root Cause
The leading cause of many uterine issues is the dominance of estrogen. Often causes fibroids, endometriosis, PMS, ovarian cysts, painful periods, and other "benign" disorders. The most usual treatment in these cases is hysterectomy.
Estrogen dominance may occur due to hypothyroidism or PCOS. Even your everyday lifestyle choices are essential in causing hormonal imbalance, such as poor diet, stress, lack of sleep, environmental toxins, poor detoxification, etc.
By making specific lifestyle changes, a woman can avoid hysterectomy and live a fulfilling life:
● Have detoxification of your body by eating healthy food & juices.
SHE TO METHOD is fundamental!
● Decrease estrogen intake by abstinence from oral hormone replacement therapy and oral contraceptives.
● To help regulate estrogen in your body, consider bio-identical progesterone by having proper sleep & diet.
● Maintain a healthy weight and improve insulin sensitivity.
● Manage your stress and control the cortisol by doing fun activities & exercises.
● Consume adaptogens to help your body deal with stress.
● Concentrate on pelvic health by doing kegel exercises to strengthen pelvic muscles and proper diet.
● Have consistent tests such as hormones, ultrasound etc., for early detection & to maintain a healthy lifestyle.
There are also Hysterectomy alternatives for non-cancer-related problems:
Hormone therapy
- Contraceptive medications and long-acting progestational agents (Implanon or Depo-Provera): These options do not appeal to me because they pose additional concerns. It's advisable not to use them if you don't need them for contraceptives.
- Antifibrinolytic medication such as Tranexamic acid (Lysteda): Tranexamic acid is an oral medication that helps control heavy menstrual bleeding.
- Gonadotropin-releasing hormone (GnRH) agonists: It's a successful treatment for women with fibroids who have bleeding symptoms; in most cases, it causes amenorrhea and reduces fibroid volume by 35-65% in a short time.
- Aromatase Inhibitors: It has fewer adverse effects than GnRH agonists and can reduce fibroid growth.
- Progesterone Modulators (Mifepristone): To reduce the growth and symptoms of fibroid tumours.
Medical interventions
For uterine prolapse or pelvic relaxation:
- Bio-identical vaginal testosterone/DHEA: Consult a functional medicine specialist to see whether vaginal testosterone/DHEA could help your situation. I discovered that it helped individuals with pelvic prolapse, incontinence, and other issues.
- Anterior and posterior repair: It repositions and restores normal functions of the pelvic organs by tightening the support tissues in place.
- Paravaginal repair: The procedure attaches the bladder and urethra to the pelvic side walls, allowing them to return to their normal position.
- Suspension operation: The uterus, bladder, and rectum can be lifted and reattached during this treatment.
- Sacral colpopexy: This surgery uses a surgically implanted synthetic mesh to maintain the vaginal wall following pelvic organ prolapse.
- Vaginal pessary: A pessary is a diaphragm-like device placed into the vaginal canal to keep the uterus in place. It is favoured when a woman is not a good surgical candidate, although it is not optimal for the long run.
For the treatment of endometriosis or pelvic discomfort:
— Bio-identical hormone vaginal therapy.
— Low-dose progestin intrauterine devices (IUDs, including Mirena, Skyla, Liletta, and Kyleena): These are birth control IUD drugs that are still systemic but have lower circulating levels than oral hormone treatment (birth control pills) and don't contain estrogen.
They're an excellent alternative to a hysterectomy. As mentioned before, I am a huge proponent of avoiding synthetic Hormone therapy and addressing the root cause of the problem.
— Laparoscopic surgery to treat endometriosis: The operation can remove endometriosis-related growths or scar tissue while keeping the uterus and ovaries without affecting the ability to get pregnant.
If you have significant bleeding or symptomatic fibroids, you should:
-Bio-identical progesterone
— Low-dose progestin intrauterine devices
— Dilation and curettage (D & C): It removes the uterine lining when it has gotten excessively thick, has heavy bleeding, or has noncancerous growths or polyps.
— Endometrial ablation: It's a procedure to stop heavy or long-term vaginal bleeding. In this procedure, the uterus lining is frozen, heated, or microwaved to destroy it. After this treatment, a woman will not be able to conceive.
— Uterine artery embolisation: The uterine arteries are embolised during this treatment conducted by radiologists (which means the blood vessels of the fibroids are blocked, causing the fibroids to shrink). After this surgery, pregnancy is not advisable, and early menopause is a known adverse effect.
— Focused ultrasound surgery using magnetic resonance guidance: This type of outpatient targeted ultrasound surgery can be used to eliminate specific fibroids. Women can still get pregnant, and the medication appears to preserve ovarian function in the long run.
— Fibroid removal by Myomectomy: Numerous approaches can be applied (abdominal, laparoscopic, hysteroscopic). While myomectomy has a similar symptom-resolution rate as hysterectomy, fibroid recurrence is possible.
— Myolysis: The surgeon reduces fibroids by heating them, commonly done laparoscopically.
I believe health is your birthright, and you deserve better choices than only removing the uterus, which may not even address your problem's ROOT CAUSE.
To avoid hysterectomy, Truhealing offers multiple treatment programmes. We even provide post-hysterectomy treatment to cope with the physical & mental challenges a patient feels after the surgery. We at Truhealing would love to be a partner in that new direction of healing.
FAQs
Originally published JUNE 27, 2022 by Dr Disha Sridhar
- Menstrual Cycles as a Fifth Vital Sign - nichd.nih.gov https://www.nichd.nih.gov/about/org/od/directors_corner/prev_updates/menstrual-cycles
- Genes control the cessation of a woman's reproductive life - National Library of Medicine https://pubmed.ncbi.nlm.nih.gov/9626112/
- Mortality Toll of Estrogen Avoidance: An Analysis of Excess Deaths Among Hysterectomized Women Aged 50 to 59 Years - https://ajph.aphapublications.org/doi/abs/10.2105/AJPH.2013.301295
- Selective progesterone receptor modulators (SPRMs): progesterone receptor action, mode of action on the endometrium and treatment options in gynecological therapies - National Library of Medicine https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4989858/
- Intravenous leiomyomatosis treated with radical hysterectomy and adjuvant aromatase inhibitor therapy - National Library of Medicine https://pubmed.ncbi.nlm.nih.gov/27436168/
- Gonadotropin-releasing hormone agonist use before hysterectomy - National Library of Medicine https://pubmed.ncbi.nlm.nih.gov/8203435/
- Antifibrinolytics for heavy menstrual bleeding - National Library of Medicine https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6494516/

- Quick Links
- Fitness
- Fertility
- Faith
- Truhealing Blogs
- Get In Touch
-
NP 404, Shriram Spandhana Challaghatta, Murugeshpalya Bangalore, Karnataka - 560037
- [email protected]
- +91 8792201157